
Why Cholesterol Climbs in Midlife for Women — And What It’s Really Trying to Do

As women enter perimenopause and menopause, one of the most common and confusing lab changes is a rise in cholesterol. Total cholesterol increases. LDL often rises. Sometimes triglycerides shift. And many women are told the same thing:
“You need a statin.”
But before we medicate a number, we need to understand what is happening biologically: This is not random. It is not a sudden moral failure of diet. And it is not simply “aging.” There is physiology behind it.
Let’s walk through it carefully and transparently.
Cholesterol Is the Foundational Building Block of All Steroid Hormones
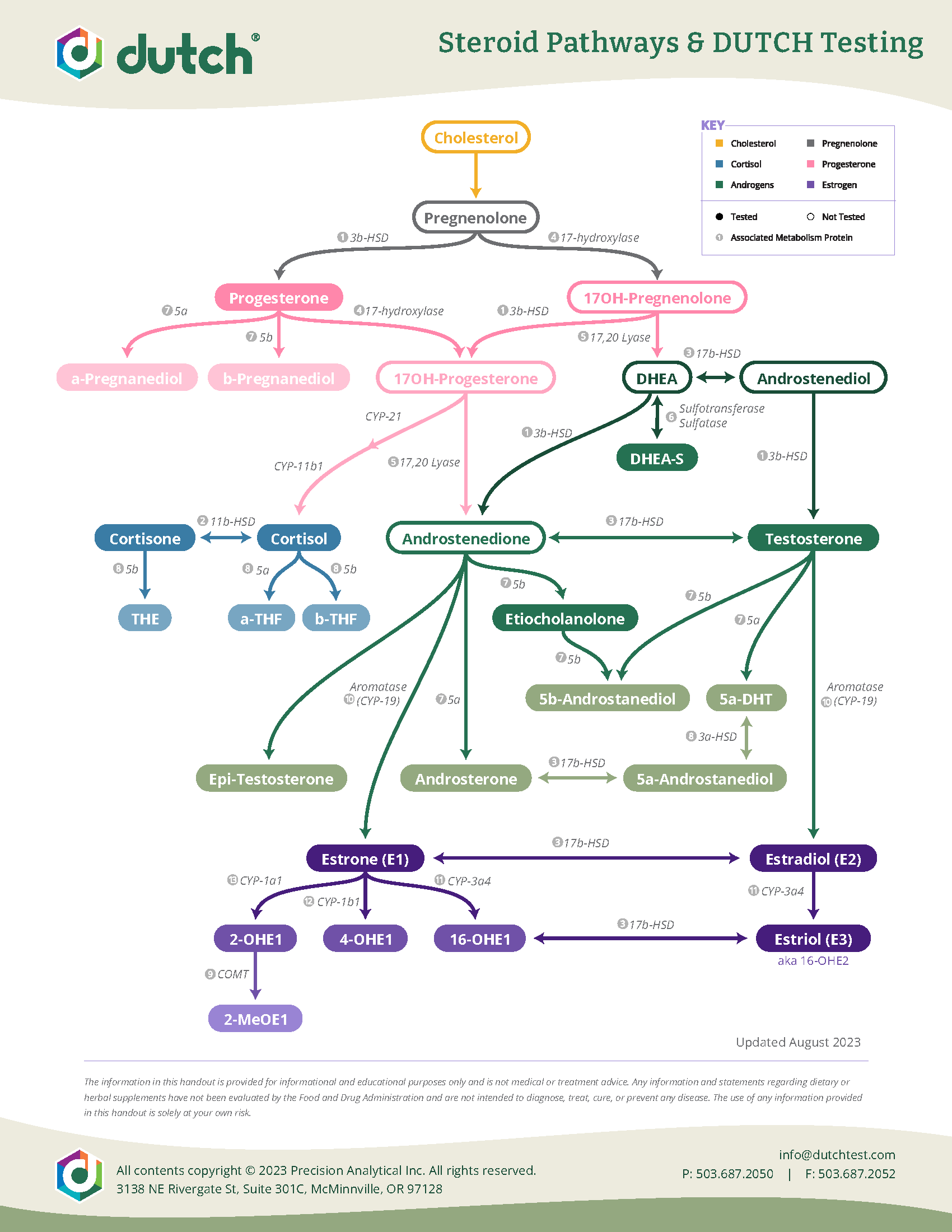
The Dutch Test Allows us to test your hormones to see how you are metabolizing them!
Cholesterol is not just a cardiovascular risk marker. It is a structural molecule essential for life.
Biochemically, cholesterol is the precursor to all steroid hormones:
Estrogen
Progesterone
Testosterone
Cortisol
DHEA
As you can see on the image of the Steroid Metabolism Pathways, the steroidogenesis pathway begins with cholesterol converting to pregnenolone, which then branches into glucocorticoids, mineralocorticoids, and sex hormones.
This is established human biochemistry and is described in standard endocrine physiology texts and reviews (Miller & Auchus, Endocrine Reviews, 2011).
Without cholesterol, steroid hormone production is impossible.
What Happens in Midlife?

During reproductive years, ovaries actively produce:
Estradiol
Progesterone
Testosterone (in smaller amounts)
As ovarian function declines in perimenopause and menopause:
Estradiol drops
Progesterone drops (often first and most dramatically)
Ovarian androgen production decreases
Now here is the critical connection:
Estrogen plays a direct role in regulating lipid metabolism. According to multiple studies:
Estrogen upregulates LDL receptors in the liver
This increases LDL clearance from circulation
Estrogen also increases HDL levels
When estrogen declines:
LDL clearance decreases
LDL particles remain in circulation longer
Total cholesterol and LDL rise
This mechanism is well documented in clinical literature, including the Study of Women’s Health Across the Nation (SWAN) and large observational cohorts (Matthews et al., Journal of Clinical Endocrinology & Metabolism, 2009).
In fact, LDL cholesterol rises by approximately 10–15% across the menopausal transition on average.
This is not speculative. It is measured longitudinal data.
Why the Body May Increase Cholesterol When Hormones Decline
Now we move into a more nuanced discussion. Biochemically, cholesterol is required to produce steroid hormones.
When ovarian hormone production declines, the body relies more heavily on:
Adrenal steroidogenesis
Peripheral tissue conversion (fat, skin, brain)
It is reasonable — and supported mechanistically — that the body maintains adequate cholesterol substrate to support steroid hormone synthesis in peripheral tissues.
There is no definitive randomized trial proving that cholesterol rises because the body is attempting to compensate for declining ovarian hormones.
What IS clearly established:
Estrogen loss impairs LDL clearance.
Cholesterol is required for steroid hormone production.
Lipid profiles worsen during menopause independent of weight gain.
The compensatory hypothesis is biologically plausible but not conclusively proven in isolation.
Are Statins Always the Best Option?

Statins reduce LDL cholesterol by inhibiting HMG-CoA reductase, the rate-limiting enzyme in cholesterol synthesis.
They are highly effective at lowering LDL levels. However, the question is not whether statins lower cholesterol. They do.
The question is whether they are always the optimal first-line intervention in midlife women with new-onset moderate LDL elevation and low overall cardiovascular risk.
Important facts from the literature:
In secondary prevention (existing cardiovascular disease), statins clearly reduce mortality.
In primary prevention for low-risk women under 65, mortality benefit is modest and sometimes statistically limited (Cholesterol Treatment Trialists’ Collaboration, Lancet, 2015).
Additionally:
Women are underrepresented in many statin trials.
Statins can reduce CoQ10 levels.
Some women report muscle symptoms, fatigue, or glucose elevation.
None of this means statins are inappropriate. It means risk stratification matters.
A woman with:
High LDL but low ApoB
Low hs-CRP
Low coronary calcium score
Good metabolic markers
…may require a different conversation than someone with diabetes, hypertension, and vascular disease. Precision medicine matters.
Can Balancing Hormones Improve Cholesterol?
Now we move to one of the most important and evidence-supported points.
Hormone therapy (when appropriately prescribed and monitored) has documented effects on lipid profiles.
Research shows:
Oral estrogen lowers LDL and raises HDL. (Bioidentical forms only please…)
Transdermal estrogen improves lipid metabolism with less impact on clotting factors.
Progesterone does not negate estrogen’s LDL-lowering effect when bioidentical micronized progesterone is used.
Meta-analyses demonstrate that menopausal hormone therapy reduces LDL by approximately 10–15% depending on formulation and route (Godsland, Climacteric, 2001; Stevenson et al., Menopause, 2004).
Additionally, balanced hormones often improve:
Visceral fat accumulation
Insulin sensitivity
Inflammation
All of which influence lipid metabolism.
When we restore physiologic hormonal signaling, lipid metabolism frequently improves without directly targeting cholesterol synthesis.
Where GLP-1 Agonists Fit In
GLP-1 receptor agonists (such as semaglutide and tirzepatide) are incretin-based therapies originally developed for diabetes and now used in obesity medicine.
They:
Improve insulin sensitivity
Promote weight loss
Reduce visceral fat
Lower triglycerides
Often reduce ApoB and LDL modestly
Clinical trials (STEP trials, SUSTAIN trials) show:
Significant weight reduction
Improvements in triglycerides
Modest LDL reductions
Reduction in inflammatory markers
Additionally, the SELECT trial (2023) demonstrated cardiovascular event reduction in overweight patients without diabetes treated with semaglutide.
This is major data.
GLP-1 therapy addresses:
Insulin resistance
Central adiposity
Inflammation
All of which influence lipid metabolism. In midlife women with:
Rising LDL
Increasing waist circumference
Insulin resistance
GLP-1 therapy may improve cardiometabolic risk markers beyond what statins alone address.
A More Integrated Model
Instead of reflexively suppressing cholesterol production, we can ask: What is driving the shift?
Common contributors in midlife women:
Estrogen decline
Progesterone deficiency
Sleep disruption
Rising cortisol
Insulin resistance
Loss of lean muscle mass
Increased visceral adiposity
When we address:
Hormonal balance
Muscle preservation
Insulin sensitivity
Inflammation
Body composition
Cholesterol often normalizes or improves significantly.
Not always. But often.
The Takeaway
Cholesterol is not the villain. It is a molecule with essential biological functions.
In midlife women:
Hormone decline alters lipid metabolism.
LDL commonly rises during the menopausal transition.
Statins reduce LDL but may not address root physiology.
Hormone optimization can improve lipid profiles.
GLP-1 therapy can further enhance cardiometabolic health.
The key is individualized risk assessment. Look at:
ApoB
LDL particle number
hs-CRP
Fasting insulin
Coronary calcium score
Family history
Then decide.
Midlife is not a disease state, it is a transition. And cholesterol may be telling a deeper story.

Why Work With Vitality Collective?
If your cholesterol has climbed in midlife, the answer is not always “just take a statin.”
And it is also not “ignore it.” The answer is precision. At Vitality Collective Hormone Health, we do not treat numbers in isolation. We evaluate the full physiologic landscape.
That includes:
Advanced lipid markers (ApoB, LDL-P when indicated)
Inflammatory markers such as hs-CRP
Fasting insulin and metabolic markers
Thyroid function
Sex hormone levels
Body composition and visceral adiposity
Sleep, stress, and lifestyle drivers
We separate:
What is hormonally driven
What is metabolically driven
What is inflammatory
What is genetically influenced
Then we build a plan. For some women, that includes:
Bioidentical hormone optimization
Structured nutrition targeting insulin resistance
Strength-based muscle preservation protocols
GLP-1 therapy when clinically appropriate
Strategic supplementation
And when indicated, collaboration with cardiology for medication management
Our goal is not simply lowering cholesterol.
Our goal is reversing metabolic dysfunction. There is a difference.Lowering LDL without improving insulin resistance, inflammation, muscle mass, and hormonal balance does not fully change long-term trajectory.
When we restore:
Estrogen signaling
Metabolic flexibility
Lean muscle mass
Insulin sensitivity
We frequently see improvements in:
LDL
Triglycerides
Inflammatory markers
Energy
Body composition
This is not a quick fix. It is structured, data-driven, medically collaborative care.
If you are in midlife and watching your labs shift in ways that feel confusing or alarming, you do not have to navigate that alone.
If you want help lowering cholesterol intelligently — and addressing the root drivers of metabolic dysfunction — we are here.
At Vitality Collective, science meets holistic physiology.
And your numbers finally make sense.
Not medical advice
This blog is for education only and is not medical advice. Supplements can interact with medications and medical conditions. Always talk with your licensed clinician before starting or changing a supplement routine—especially if you are pregnant, breastfeeding, managing a chronic condition, or taking prescription medications.
If you want more information or support, book a free 20 minute wellness consultation with us - call 844-662-3288 or book online.